
Arrhythmia and AF Clinic

What are the types of arrhythmias ?
The types of arrhythmias include:
- Supraventricular arrhythmia (arrhythmia originating from atria – upper chambers)
- Premature atrial contractions (PACs).
- Atrial fibrillation.o Atrial flutter.
- Paroxysmal supraventricular tachycardia (PSVT).
- Associate with accessory pathway
- Associate with AV node only
- Atrial tachycardia
- Sinus node dysfunction
- Ventricular arrhythmia (arrhythmia originating from ventricle – lower chambers)
- Premature ventricular contractions (PVCs).
- Ventricular tachycardia (V-tach).
- Ventricular fibrillation.
- Brady-arrhythmias.
- Heart block.
- Arrhythmia associate with specific condition
- Long QT Syndrome
- Brugada
- Arrhythmogenic right ventricular dysplasia (ARVD)
- Premature atrial contractions. These are early extra beats that originate in the atria (upper chambers of the heart). They are harmless and do not require treatment.
- Atrial fibrillation. Atrial fibrillation is a very common irregular and fast heart rhythm that causes the atria, the upper chambers of the heart, to become quivering. The ventricles, the lower chambers will usually beat fast unless there are controlled by medication. Atrial fibrillation can be terminated with medications or direct current cardioversion. Radiofrequency ablation technique is more effective than medication.
- Atrial flutter. This is an arrhythmia caused by one or more rapid circuits in the atrium. Atrial flutter is usually more organized and regular than atrial fibrillation. It often converts to atrial fibrillation.
- Paroxysmal supraventricular tachycardia (PSVT). A rapid heart rate, usually with a regular rhythm, originating from above the ventricles. PSVT begins and ends suddenly. There are two main types: accessory path tachycardia and AV nodal reentrant tachycardia (see below).
- Accessory pathway tachycardia. A rapid heart rate due to an extra abnormal pathway or connection between the atria and the ventricles. The impulses travel through the extra pathways as well as through the usual route in a circle causing the heart to beat fast.
- AV nodal reentrant tachycardia. A rapid heart rate due to more than one pathway through the AV node. In many cases, like the accessory pathway tachycardia, it can be terminated using a simple maneuvers, such as breathing in and bearing down, and others performed by a trained medical professional. Some drugs can also stop this heart rhythm. As with other tachycardia, it can be treated effectively with radiofrequency ablation technique.
- Premature ventricular contractions (PVCs). These are among the most common arrhythmias and occur in people with and without heart disease. This is the skipped heartbeat we all occasionally experience. In some people, it can be related to stress, too much caffeine or nicotine. But sometimes, PVCs can be caused by heart disease or electrolyte imbalance. People who have a lot of PVCs, and/or symptoms associated with them, should be evaluated by a heart doctor. However, in most people, PVCs are usually harmless and rarely need treatment.
- Ventricular tachycardia (V-tach). A rapid heart rhythm originating from the lower chambers (ventricles) of the heart. The rapid rate prevents the heart from filling adequately with blood; therefore, less blood is able to pump through the body. This can be a serious arrhythmia, especially in people with heart disease, and may be associated with more symptoms. A heart doctor should evaluate this arrhythmia.
- Ventricular fibrillation. An erratic, disorganized firing of impulses from the ventricles. The ventricles quiver and are unable to contract or pump blood to the body. This is a fatal arrhythmia and a medical emergency that must be treated with cardiopulmonary resuscitation (CPR) and defibrillation as soon as possible.
- Long QT syndrome. The QT interval is the area on the electrocardiogram that represents the time it takes for the heart muscle to contract and then recover, or for the electrical impulse to fire impulses and then recharge. When the QT interval is longer than normal, it increases the risk for “torsade de pointes,” a life-threatening form of ventricular tachycardia. Long QT syndrome is an inherited condition that can cause sudden death in young people. It can be treated with antiarrhythmic drugs, pacemaker, electrical cardioversion, defibrillation, implanted cardioverter /defibrillator, or ablation therapy. This condition is not common.
- Brugada syndrome. The Brugada syndrome is a genetic disease that is the major cause of sudden cardiac death in young men without known underlying cardiac disease in Southeast Asia such as Thailand and Laos. It has characteristic abnormal electrocardiographic (ECG) ST elevation in early precordial leads. It is named by the Spanish cardiologists Pedro Brugada and Josep Brugada.
- Brady-arrhythmias. These are slow heart rhythms, which may arise from disease in the heart’s electrical conduction system. Examples include sinus node dysfunction, (Atrioventricular) heart block and medicine side effect.
- Sinus node dysfunction. A slow heart rhythm due to an abnormal (SA) sinus node. Significant sinus node dysfunction that causes symptoms is treated with a pacemaker.
- Heart block (Atrioventricular). A delay or complete block of the electrical impulse as it travels from the sinus node to the ventricles. The level of the block or delay may occur in the AV node or HIS-Purkinje system. The heart may beat slowly. If serious, heart block is treated with a pacemaker.
How are arrhythmias diagnosed?
Electrocardiogram (ECG, EKG)

Regular
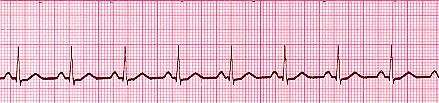
Tachycardia (Regular)

Bradycardia

Irregular

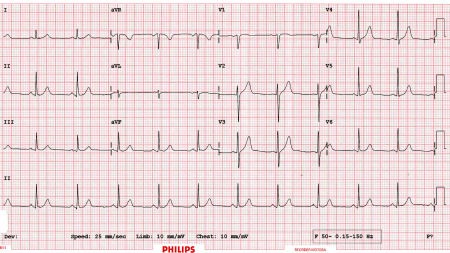
12 Leads ECG
For more information, please contact
Arrhythmia and AF Clinic
2nd Floor, H Building, Bangkok Heart Hospital